



Who Actually Runs Health in China? A Map of Policy and Power
Your foundational explainer to China’s health governance, and how the many pieces fit together to direct care, cost and access.

🩺 This Vital Signs post at China Health Pulse provides an overview of China’s current health ministries: who does what, where the power sits, and why it’s not as simple as a single authority.
A System Without a Centre
In China’s health system, governance truly matters more than anything else. The shape of policy architecture doesn’t just influence the public system; it defines the rules, boundaries and incentives of the private market too. Even in sectors where the pace of digital innovation or biotech R&D can move quickly towards commercialisation, alignment matters more than data or product, and survival (let alone success) is fully dependent upon reading policy signals and navigating institutional relationships.
Understanding health governance in China is essential. But it’s complex and distinctive.
Governance fragmentation is not unique to China. The US splits power across CMS, FDA, CDC and NIH among others. The UK separates policy from provision, devolves power across four nations, and maintains agencies for licensing, pricing and regulation. The same goes for every country in Europe, and really, around the world.
What is unique to China’s strategic jigsaw, however, is is how flat the hierarchy runs. Reporting lines are diffuse, and power flows not only from the State Council but through Party commissions, local Party secretaries and long-standing institutional momentum.
There’s also deliberate decoupling: where top-down policy drive is combined with bottom-up decentralised execution to produce regional variations in access, outcomes and speed of reform. National agencies set frameworks and launch pilots, but they cannot directly enforce uniform execution. Implementation on the ground depends on local finances, reform incentives and provincial leadership (I’ve written about this before). This means that what happens in clinics and hospitals (and hence, what patients actually experience) varies dramatically across geography.
Understanding who does what and why requires tracing both the architecture and the incentives.
This post provides a starter map, setting out the ecosystem as it stands in 2025: who the major players are, what they’re responsible for, and how they interact. In future Real Diagnosis posts, I’ll go deeper into key ministries to explain their history and trajectory - as well as anecdotes from my time working with them
How We Got Here
China’s current health system fragmentation is the product of deliberate reform. Each major reorganisation reflected a political priority of the time, responding to rising costs, slow approvals, data fragmentation or lack of preparedness, to create new boundaries that influence how power and policy flow now. But the cumulative effect has been to split strategic direction from operational control.
In the Maoist decades of the 1950s onwards, health was centrally planned, with a focus on rural service delivery and public campaigns. From the 1980s, as economic reform took hold, and China opened up under Deng, hospitals became commercialised and local governments gained more autonomy over service provision. Central control weakened.
The 2003 SARS outbreak triggered an overhaul of disease surveillance, and in 2009, after a series of vaccine scandals, China’s first major health reform package expanded basic insurance and introduced an essential drug access system.
In 2013, health and family planning were merged into a single commission (an uneasy fusion that reflected the political fading of the one-child policy) but by 2018, that body was dissolved and its functions scattered. Pricing moved to one agency, regulation and insurances to others, and epidemic control reshuffled — including yet again in 2022 after COVID.
Each split has served a purpose: to contain costs, improve oversight or accelerate innovation. But the result is a system where no single body holds all the levers, and where coordination is as much a political exercise as a technical one.
Who Does What: Quick Profiles
Before reviewing the main shortlist, it’s important to be aware that, unlike many systems run by generalist civil servants in other countries, China’s health governance is deeply technocratic. Surgeons, epidemiologists, statisticians and systems engineers lead at the helm.
This technocratic DNA means that what may looks chaotic from the outside is actually coordinated complexity. It explains how policy is written: less politicised and often cautious, jargon-heavy and implementation-obsessed. It also explains why systems thinking and pilot-based experimentation dominate reform logic, whether in reimbursement or regulatory alignment.
I've linked below to official websites where possible. Do note which are in English, and which are not: whether by design or inertia, most of that linguistic opacity is strategic.
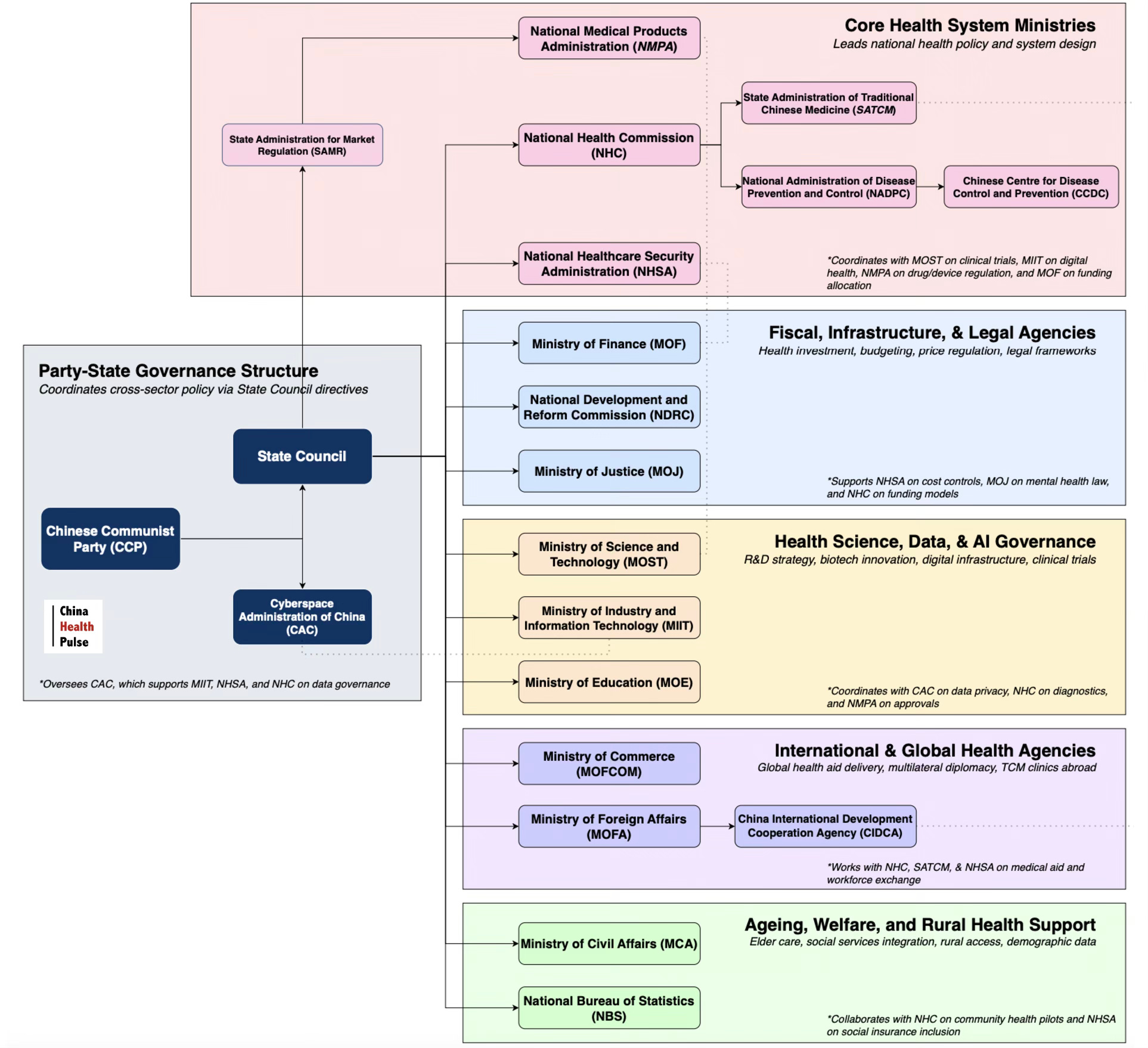
OVERSIGHT: The State Council is China’s main administrative body (perhaps similar to a cabinet), signing off on budgets, approves reforms, and coordinates between most health ministries. It reports into the Communist Party, which sets political direction.
SYSTEM: The National Health Commission sets the tone. It leads on public health strategy, reform pilots, hospital oversight and the Healthy China 2030 blueprint. But it no longer controls funding or market access, and so its authority is becoming more symbolic, strategic and negotiable.
REIMBURSEMENT: Money determines access. The National Healthcare Security Administration manages insurance funds, sets drug prices, updates the National Drug Reimbursement List and leads payment reform. It is arguably the most powerful player in the system today.
REGULATION: The National Medical Products Administration, China’s FDA/MHRA/EMA, regulates drug and device approvals to ensure safety and efficacy. It ensures safety and efficacy and reports via State Administration for Market Regulation. It is global-facing but structurally separate.
SURVEILLANCE: The National Administration for Disease Prevention and Control was created post-COVID, after the Centre for Disease Control failed to manage pandemic spread and control. Its purpose is epidemic command, but so far, it seems to have added more layers than clarity.
INNOVATION: The Ministry of Science and Technology and Ministry of Industry and Information Technology together steer China’s health innovation strategy, from AI diagnostics to precision medicine. Their role in health is indirect but powerful, especially as China aims to grow domestic research and reduce dependency on global platforms. The Cyberspace Administration of China governs health data, shaping how platforms collect, share and export sensitive information. Their roles are indirect, but increasingly decisive.
GLOBAL HEALTH: I’ve written before how China International Development Cooperation Agency (equivalent of USAID) leads on China’s health aid, working with NHC and Ministry of Foreign Affairs to deliver South-South partnerships, including medical aid, health infrastructure projects, pandemic response partnerships and health diplomacy.
LEGAL & WORKFORCE: The Ministry of Justice drafts health laws on data, mental health, patient rights and insurance oversight. The Ministry of Education oversees licensing and training standards for doctors, nurses and public health workers. Together, they govern who is allowed to practise and and under what rules.
A Dense Web
These many health and health-related agencies hold overlapping mandates and cross-cutting incentives. Some of these roles are formally named, but many are not, and there are real drawbacks to this model. Authority can be siloed, co-ordination can slow, and bureaucracy can add friction.
When I worked with these various bodies in my time leading the health team at the British Embassy in Beijing, I often found myself relaying between ministries that didn’t talk to each other. A reimbursement question could lead to a regulator, who pointed to a local pilot site, who then circled back to national planners.
And yet, China moves, because each agency is under real pressure to deliver. Reform is demanded from the top down, and what takes other countries years to test, China often pilots and scales in less than five. Within the span of two decades, the country has transformed from a fragmented health landscape of rural gaps and underfunded hospitals, to a system that remains uneven in places, but is also more integrated, technologically advanced and ambitious than ever before.
In upcoming posts, I plan to take a closer look at the key players, including the National Health Commission (NHC), the National Healthcare Security Administration (NHSA), and the National Medical Products Administration (NMPA). Together, they determine what care is offered, what treatments are reimbursed and what innovation reaches patients. I will also be unpacking the policy frameworks that define China’s health ambitions, including Healthy China 2030, the National Drug Reimbursement List, and broader national priorities on digital infrastructure and system reform.
Yes, this system is fragmented. But it is far from aimless. And looking beyond what seems opaque and confusing to learn how it really works, is the first step to understanding where it’s headed next - whether you are in industry, policy, research or global health.
🩺 This Vital Signs post at China Health Pulse provides an overview of China’s current health ministries: who does what, where the power sits, and why it’s not as simple as a single authority. In upcoming Real Diagnosis posts, I’ll dive deeper into the histories and responsibilities of the major bodies that leads China’s system reform, innovation, regulation and reimbursement.
Related posts:
Five Biggest Myths I See About China’s Healthcare

Here’s what everyone keeps getting wrong - and why it really matters.
Health and the Two Sessions (Pt 1 of 2): What China’s Top Political Event Really Revealed This Year

China’s Two Sessions each March is a political mega-event. It’s more than the King’s Speech or State of the Union combined—where top policymakers set up the year through suits, slogans and symbolism.
No, China Won’t Replace USAID. But Here Are Five Ways It's Rewriting the Global Health Playbook.

As Western donors retreat, many fear that China will fill the gaps and disrupt the global health order. But in practice, China offers fresh, alternative tools, and the Global South is listening.
Thanks Ruby- this is very insightful. As you eluded to, China's very centralised agenda setting and the sheer efficiency extend well beyond healthcare. For example, the Air Pollution Prevention and Control Action Plan (APPCAP) in 2013 with legally binding air pollution (PM2.5) targets, that led to PM2.5 concentrations to fall to 1/3 within a space of 5 years. The Ministry of Ecology and Environment used central coal-to-industry price controls but there was also fierce inter-regional competition to accelerate vehicle-emission standards, and clean-fuel rollouts.
In context the air pollution reductions in China far outpace similar Clean Air Acts introduced in the US and UK, which took 30+ years to achieve similar gains.
This is thorough and useful but what about the PLA?